AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2642-9756/026
1 Lecturer of Obstetrics and Gynecology, Faculty of Medicine, Benha University, Benha, Egypt.
*Corresponding Author: Waleed Tawfik, Lecturer of Obstetrics and Gynecology, Faculty of Medicine, Benha University, Benha, Egypt.
Citation: Waleed Tawfik(2020) Assessment of different management options used in morbidly adherent placenta and pregnancy outcomes. J Women Health Care and Issues, 3(2): Doi:10.31579/2642-9756/026
Copyright: © 2020.Waleed Tawfik. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 March 2020 | Accepted: 04 April 2020 | Published: 10 April 2020
Keywords: morbidly adherent placenta; pregnancy; hemostatic sutures
The aim of this work is evaluation of different management options for patients with morbidly adherent placenta and its effect on pregnancy outcomes to find the best method of management to decrease morbidity and mortality. In this prospective study, there were 42 patients diagnosed as having morbidly adherent placenta previa and hospitalized between January 2019 to February 2020.
Different management options performed to patients with morbidly adherent placenta previa were recorded, blood loss was estimated for each patient, operative procedures, maternal and fetal outcome was recorded.
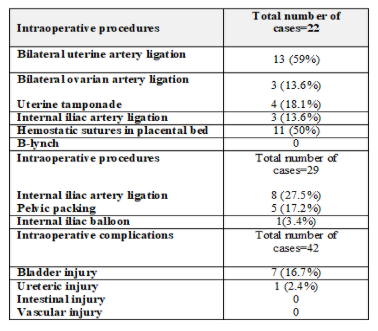
The results showed the following: Different methods were tried to preserve the uterus including bilateral uterine artery ligation in 13 (59%) cases, bilateral ovarian artery ligation in 3 (13.6%) cases, bilateral internal iliac artery ligation in 3 (13.6%) cases, intrauterine tamponade in 4 (18.1%) cases and hemostatic sutures in placental bed in 11(50%) cases, while B-lynch suture was not done, while procedures which were performed to control pelvic hemorrhage after hysterectomy included internal iliac artery ligation in 8 (27.5%) cases, pelvic packing in 5 (17.2%) cases and internal iliac balloon inflation to control hemorrhage in 1 (3.4%) case.
The postoperative complications were DIC occurred in 2 patients (4.8%), ICU admission occurred in 5 cases (11.9%), two cases required reoperations, one patient (2.4%) had wound infection, Postpartum collapse occurred in 2 case (4.8%). Pulmonary embolism occurred in 1 case (2.4%), Median duration of hospital stay was 4 days (range: 2-25).
The greatest challenge in modern obstetrics remains the morbidly adherent placenta (MAP). At the time of placental separation, the maternal risk tends to result in extreme hemorrhage, disseminated intravascular coagulation (DIC), significant need for blood transfusion, intensive care, hysterectomy and sometimes maternal death [1,2].
A multidisciplinary approach is important in treating these patients to reduce MAP-associated morbidity and mortality. The anticipation and management of major hemorrhage, including the availability of packed cells, platelets, fresh frozen plasma, cryoprecipitate and activated factor VII, should be given special consideration. The technology of interventional radiology [3].
Balloon catheter Occlusion of the pelvic arteries or Selective Arterial Embolization reduces blood flow to the uterus and allows surgery to be conducted in simpler and more controlled conditions. Until peripartum hysterectomy, bilateral internal iliac artery ligation is performed in an effort to reduce the surgical blood loss. This is particularly relevant in circumstances where interviews take place [4].
Few other surgical approaches have been identified, including a hysterectomy, to achieve hemostasis in MAP cases. You may "excision the placental spot" If the placental attachment region is focal and the majority of the placenta is removed, then a "wedge resection" of the region can be carried out [5,6].
The goal of this research is to examine various management methods for patients with morbidly adherent placenta and their impact on pregnancy outcomes in order to find the best management approach for decreasing
.MAP-related morbidity and mortality
Patients and Methods:
The present study is a prospective study for pregnant women who were diagnosed as morbidly adherent placenta and hospitalized between January 2019 to February 2020 at the Obstetrics and Gynecology Department, Benha University. Egypt
Inclusion criteria:
All cases of placenta previa in the third trimester admitted to Zagazig University Hospitals and diagnosed antenatally as morbidly adherent placenta.
Exclusion criteria:
Any medical disorder with pregnancy as anemia, hypertension, diabetes, cardiac lesion, liver diseases or kidney diseases.
Sample size:
The total number of morbidly adherent placenta previa cases admitted to Hospitals per month about 7 cases, so all admitted cases during the period of the study were included equal 42 cases.
Each woman was subjected to the following:
Examination:
General examination:
Abdominal examination:
Laboratory investigations:
A blood sample was withdrawn to check for complete blood count, coagulation profile, liver function tests, renal function tests and random blood sugar.
A urine sample was taken to check for proteinuria, hematuria and presence of urinary tract infection.
Blood group, cross matching for blood and plasma before operation
Ultrasound:
Ultrasound was performed for each patient to confirm viability, gestational age, fetal biometry, fetal presentation, amount of liquor and detailed assessment of placental site, degree of adherence by 2D ultrasound and Doppler
Sonographic features of morbidly adherent placenta by 2D ultrasound:
Retroplacental sonolucent zone deficiency;
The lacunae vascular.
Thinning myometrials.
Bladder line breakage.
Exophytic masses present.
Characteristic findings on color Doppler ultrasound include:
A diffuse lacunar flow pattern with high-velocity pulsatile venous type flow (peak systolic velocity more than 15cm/s) spread throughout the placenta, myometrium and cervix.
A central lacunar flow pattern with turbulent flow distributed regionally or focally in the parenchyma.
Bladder–uterine serosal interphase hyper vascularity.
Markedly dilated vessels over the peripheral sub placental zone.
An absence of sub placental vascular signals in the areas lacking the peripheral sub placental hypo echoic zone.
Abnormal vascular channels linking the placenta to the bladder.
Counselling:
Counseling for the severity of the case.
Counseling about different management options up to hysterectomy.
Counseling about the gestational age of termination and possibility of incubator admission.
Counselling about the desire for future fertility.
Consenting:
An informed written consent about different management options that may reach to hysterectomy was taken from all patients and their husbands and about the need to blood and blood products during the operation and risk of mortality.
Surgical techniques:
All cases with MAP were operated by a senior obstetrician with attendance of a senior anesthesiologist.
General anesthesia was given to all patients.
Prophylactic antibiotic was given before skin incision.
Skin incision: midline or pfannenstiel incision.
Uterine incision: high transverse incision or vertical upper segment incision.
Delivery of the baby.
Hysterectomy without attempt placental removal or trial placental removal followed by conservatives' procedures was left to the experience of the senior obstetrician operating the patient.
Bilateral internal iliac ballon was inserted before operation and inflated after delivery of the baby to decrease blood loss during surgery in one case.
If bladder or ureteric injury was suspected urological consultation was done.
Postoperative care:
Complete blood count and packed RBCs transfusion if the patient was anemic.
Early mobilization, good hydration and prophylactic anticoagulant if needed to prevent DVT.
After discharge the patients returned to outpatient clinic to remove stitches and their wounds were examined for infection.
Estimation of blood loss:
Real blood loss (ABL) was estimated from a gross formula modification
Actual blood loss= BV {Hct(i) − Hct(f)}/ Hct(m) BV: volume of blood. Blood volume is determined by using the following formula, dependent on body weight. Blood volume= Body weight (in Kg) at 70 Hct(i): initial hematocrit Hct(f): final hematocrit Hct(m)
Neonatal care:
All neonates were examined by pediatrician with detection of APGAR score, gender and birth weight.
Statistical analysis:
Data collected, recorded, entered and analyzed using Microsoft Excel software throughout history, basic clinical evaluation, laboratory investigations and outcome measures. Data was then imported into the Social Sciences version 16.0 Statistical Package. (V16 SPSS). Depending on the type of qualitative data expressed as number and percentage
The present retrospective research was performed over the period from December 2018 to May 2019 on cases of morbidly-adherent placenta prioria. This research contained a total of 42 cases of morbidly-adherent placenta prioria.
as shown in table (1). Among the included 42 women with morbidly- adherent placenta previa, 20 (47.61%) cases presented with antepartum hemorrhage (APH), Among the included 42 women, morbid placental adherence by preoperative U/S was in the form of ‘focal accreta’ in 13 (31%) women, ‘accreta’ in 14 (33.4%) women, ‘increta’ in 10 (23.8%) women and ‘percreta’ in 5 (11.9%) women, as shown in table (2) Among the included 42 women with morbidly-adherent placenta previa, 14 (33.3%) cases had urgent surgery due to antepartum hemorrhage or uterine contraction, while 28 (66.7%) had elective surgery, Trial of placental removal plus application of conservative measures was done in 22 (52.4%) women that succeeded in 13 (31%) women (CS only) and
failed in 9 (21.4%) women (hysterectomy), Hysterectomy was done in 20(47.6%) women from the start without trial of placental removal, Among the included 42 women, midline incision was done in 13 (31%) cases and pfannenstiel incision was done in 29 (69%) women as shown in table (3)
Intraoperatively, removal of the placenta was tried in 22 (52.4%) cases, different methods were tried to preserve the uterus including bilateral uterine artery ligation in 13 (59%) cases, bilateral ovarian artery ligation in 3 (13.6%) cases, bilateral internal iliac artery ligation in 3 (13.6%) cases, intrauterine tamponade (uterine pack or Foley catheter) was placed in 4 (18.1%) cases and hemostatic sutures in placental bed in 11(50%) cases, while B-lynch suture was not done, Intraoperatively, procedures which were performed to control pelvic hemorrhage after hysterectomy included internal iliac artery ligation in 8 (27.5%) cases, pelvic packing in 5 (17.2%) cases and internal iliac balloon inflation to control hemorrhage in 1 (3.4%) case, Bladder injury occurred in 7(16.7%) cases and ureteric injury occurred in only 1 (2.4%) case with ureteric stent insertion, while vascular and intestinal injury did not occur as shown in table (4)
The estimated median blood loss intraoperatively was 2 L (range: 1–8 L). Both cases need transfusion into the blood. The median was four units (range: 1–17). FFP transfusion overall concentrations were 39/42 (92.85 per cent). The median was 2 units (range: 1–8 units). Only 2 (4.76 per cent) women received platelet transfusion and only 3 (7.14 per cent) women were transfused with cryoprecipitate. Only 1 (2.4%) woman needed recombinant activated factor vii due to DIC, Of the included 42 women, 2 (4.8%) cases developed DIC, 5 (11.9%) cases were admitted to
ICU postoperatively, 1 (2.4%) case developed wound infection, 1 (2.4%) case developed pulmonary embolism , 2 (4.8%) women developed postpartum collapse and 2 (4.8%) cases were re-operated again (for evacuation of hematoma and the second case for removal of abdominal packs which was left to control pelvic hemorrhage after hysterectomy) , only 1 (2.4%) case died during the study period from internal hemorrhage, According to table (5), the median hospital stay after delivery was 4 days (range: 2-25 days).
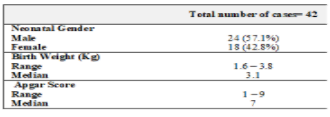
Of the 42 neonates who were included, 24 (57.1%) were males, while 18 (42.8%) were females. As shown in table (6), the median birth weight was 3.1Kg (range: 1.6–3.8Kg) and the median Apgar score was 7 (range: 1– 9).




Although, until recently, Morbidly attached placenta has been considered a relatively rare occurrence, its annual incidence seems to be rising. In 1994, the incidence of morbidly adherent placenta over the previous 10 years was estimated to be 1 in 2510 cases, while a 2002 study recorded an incidence of 1 in 533 cases over the preceding 20 years and an incidence of 1 in 210 cases in 2006 (8,9).
In the current study 42 cases diagnosed prenatal as morbidly adherent placenta, In 20(47.6%) women hysterectomy was done without trial of placenta removal, In 22(52.4%) women trial of placental removal was done preceded by uterine massage and uterotonics and followed by conservatives procedures to control bleeding from the placental bed. Due
to absence of management protocol for morbidly adherent placenta in our emergency hospital, so hysterectomy without attempt placental removal or trial placental removal followed by conservatives procedures was left to the experience of the senior obstetrician operating the patient.
Generally speaking, trial placental removal was performed in many cases mainly due to low parity of many patients and their desire for future fertility and prenatal U/S (greyscale and Doppler) not has 100
In conclusion, up till now there is not completely sensitive and specific test for the diagnosis of MAP, when morbidly adherent placenta is diagnosed or suspected antenatally, delivery should be scheduled in a tertiary care center with appropriate expertise and facilities. Generally, the recommended management is cesarean hysterectomy. However, this approach might not be considered the first line of treatment in women who have a strong desire for future fertility. Therefore, surgical management of morbidly adherent placenta may be individualized, available quantity of blood products and multidisciplinary approach may reduce maternal morbidity and mortality in these patients, Good anticipation and timely decision is the key to success in this life- threatening condition.
Recommendations:
The recommended management for morbidly adherent placenta is hysterectomy without attempt placental removal especially if there are signs of placental invasion, but in nulliparous women we recommended conservative measures to safe the uterus and no hurry for hysterectomy to give the chance for placental separation.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
